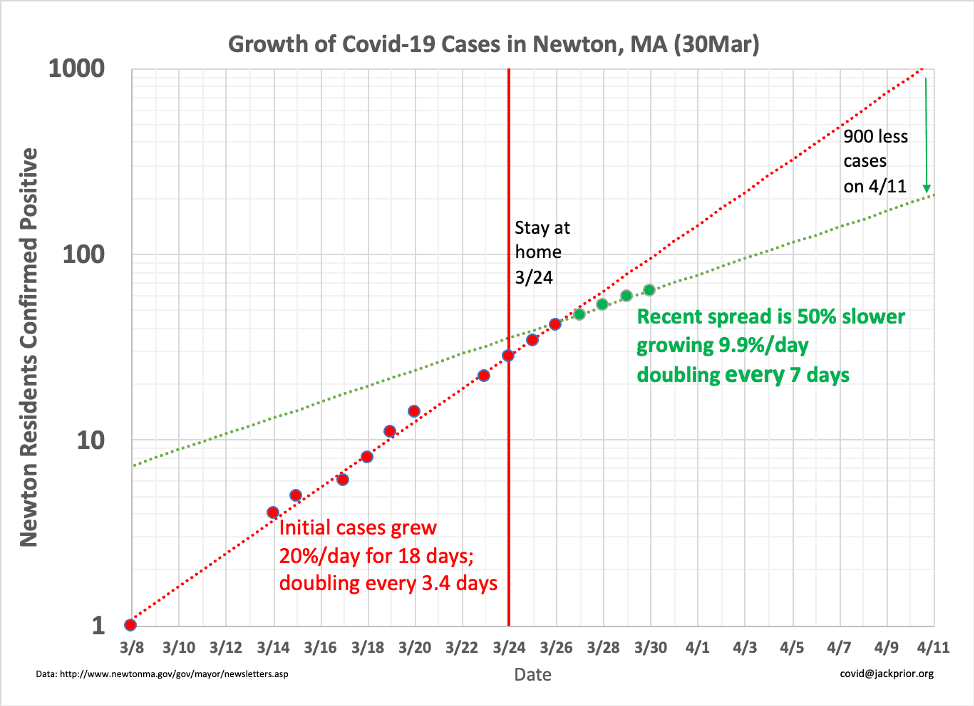
[UPDATED with new charts Jack provided in comments] Jack Prior has been analyzing data on confirmed COVID-19 cases for Newton (as well as for the U.S., China, and the world). He’s plotting the data on a logarithmic scale to show how closely it tracks with exponential curves and to make short-term projections. The bad news is that exponential growth skyrockets, and the data has been tracking that alarming growth. The good news is that in Newton, the Stay-at-Home order (or suggestion? or advice?) sure looks like it’s working to #FlattenTheCurve from when it began on March 24. Compare the red dotted line of previous experience with the green dotted line of Stay-at-Home. The rate of growth drops from around 20% per day down to around 10% per day. Morale: #StayAtHome.
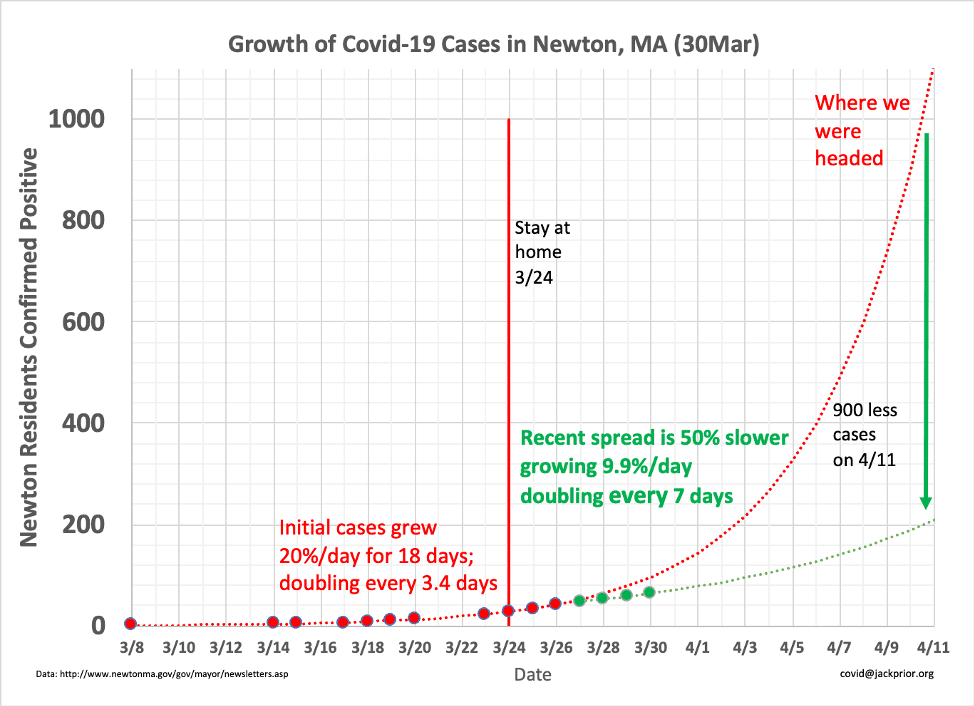
And here are the data and projections on a linear scale, to illustrate more clearly the positive impact of Stay-At-Home on reducing exponential growth:
Thanks for sharing Bruce. Let’s hope the trend continues.
Here is a cleaner version of the plot with a weekend data point added and updated projection. Stay at home has reduced the likely number of cases in Newton by 4/11 from over a 1000 to 200. That means a lot less load on the health care system and likely 80% less near term deaths. The reduction in infection rate parallels what has been seen in the Seattle area with “Stay at Home”.
https://newtonwatch.org/wp-content/uploads/2020/03/newton-covid-19-Mar30th-2.png
Here is the same graph, but on a linear scale. You can see the stark difference between where we were headed and the current trajectory we are on.
http://newtonwatch.org/wp-content/uploads/2020/03/newton-covid-19-Mar30th-2-linear.png
Thanks for creating these Jack, looking forward to updates.
@Jack Prior, thanks for the data. A couple of comments:
1. Given how spottily we test in the U.S., the number of confirmed cases is not a particularly trustworthy statistic. Here’s hoping the trend continues.
2. If the new trend is accurate, it suggests that voluntary distancing was having an impact before the stay-at-home order was implemented, given the typical 7-day incubation period. Good for the citizenry if true!
I think we should also give credit where credit is due. Closing schools when we did was a good thing. (Yes, it could have been done a little earlier, it’s not like we didn’t know where this was going. But there were reasons and it worked out.) Making restaurants take-out only was also a good thing, and done relatively early.
At the early stage of disease spread, transmission happens in discrete events that is harder to model statistically by trend lines. Had COVID-19 gotten into the schools in just the wrong way (a super spreader staff member, for instance) we could have seen a Newton hotspot emerge. Same is true at a large restaurant or buffet.
Such an event might not have changed the shape of the trend line very much, but it would have moved us up the curve. We saw this with Biogen. It would have added a lot of cases to our base infection level, which would in effect adversely multiply the impact of any of our other decisions. It would also have gotten us closer to the limits of hospital capacity faster.
Those relatively early closures gave us all time to prepare without full-blown panic.
I think you’re right, Mike. The action you mentioned (school closure on March 12 and restaurants moving to takeout on March 15) are likely important factors. Jack’s earlier chart showed these dates. These actions are key parts of the social distancing that John referred to in his point #2. It takes some days for them to have an effect on the number of confirmed positive cases, due to incubation and testing times.
Also, doing big, dramatic, and socially inconvenient things like closing schools and restaurants forced people to take things seriously. It showed the government was taking things seriously, which asserted leadership when things started to get worse.
Compare that to other governors or mayors who dithered and had to backtrack, or are still dithering. They’ve blown their preparation time and their credibility. That’s a bad combination.
We really benefit by having the world’s experts advising government and living in our community.
Oh, one more comment. There’s diffuse discussion about how we haven’t gone far enough, and how we need to ratchet up public restrictions more. I think such a step will have minimal gain from a statistical point of view.
What I think we can do at the city and state level is be more formal in our demands that essential businesses follow social distancing, hygiene protocols, and employee leave policies. My understanding is that such regulations are well within the purview of local and state health boards.
This step would help with some of the situations we’ve heard about here (landscapers with full trucks), as well as ones we have heard about nationally (Amazon workers striking because they don’t have hand sanitizer, have to work close together, and can’t take time off when sick.) These kind of situations are the ones that can produce a local hotspot, and they are already regulated and licensed by the government in some way.
To start, every essential business that wishes to remain open should have to submit a COVID-19 policies and compliance document to the city.
A tip of the hat to Jack Prior, Bruce Henderson, the City and all the residents of Newton who have heeded the warning to shelter in place. Three things we will all have to temper are battle fatigue. complacency and pressures to return things to some sense of normalcy before it is absolutely safe to do so. Everyone will feel the urge to do so. It’s in our DNA, But we have to be reasonable how we open things up as the threat starts to abate. I’m 83 with two underlying medical conditions so I know I’m toast if I get a serious case of this virus and even a moderate case. But it’s also now clear that it threatens individuals in every age group. It will be no comfort whatsoever for me or anyone else to contract a bad case of this virus a month or so down the line when the threat seems on the way out, and this virus appears to be particularly cunning and baffling.
@John White — I think we need to recognize the data has some limitations, but it is the picture we have. The case count may be off by 2 or 3x, but it is growing 10x every 2 weeks, which swamps that error. Note also that the problem in the US is as much, if not more so, the long delay in getting results. We eventually know someone is infected but its too late for containment.
The case fatality rate (CFR) in the US is 2% compared with 1.7% in South Korea, which has extensive testing. That suggests we are not that far off in knowing who is infected if, and this is a big if, we are counting all those dying from Covid19. We may be missing both. South Korea did find that 95% of people who had what seemed like clear Covid19 symptoms had something else.
The incubation period varies, but can be as quick as 2-3 days. The graph doesn’t show any bend until 3 days after the stay at home, so its not clear that school and resturant closing had much of an impact. People were getting infected at work and kids may have still been transferring in play dates.
Family transfer is probably the dominant infection source in the days after the stay at home, and may start to fade.
Very sweet. Testing really kicked in statewide on 3/22 (from 3000), so I’d guess the true bend came a little earlier (more tests yields more cases and an upward swing), and, as several have suggested, all the distancing interventions (schools, restaurants, messaging etc) contributed to the effect.
I’m curious if anyone on this thread has thoughts (and knowledge) of modeled estimates, how those have moved over time, and what proportion at each juncture are identified as confirmed cases.
One additional comment. The case fatality rate is roughly 2% in US (not per infection, but per case significant enough to be confirmed). That means the efforts we have undertaken will lead us to avoid approximately 18 resident deaths in the next several days. We are going to have deaths, but there would have been many more, and sooner without the stay at home.
Additionally, it would be great to know testing (all tests, negative as well as positive) numbers in Newton. The MA wide numbers are not encouraging; the % + is increasing day-over-day (21% yesterday up from 8% a week before), indicating that the state is still behind the epidemic’s curve.
Thanks for the follow-up, @Jack. I appreciate your showing us that distancing efforts are important and starting to bear fruit.
FYI — Today’s data point was 83 cases for 3/31, which pushes up the forecast, unfortunately. Here is the new linear graph:
http://newtonwatch.org/wp-content/uploads/2020/03/newton-covid-19-Mar31th-linear.png
From 3/20 – 3/30 we averaged 6 cases per day – and it never deviated more than a case up or down. Today it jumps 19; that could be just chance variability that looks more volatile than it really is because of the small numbers. But we really ought to be able to dig deeper behind the numbers to see if there’s an plausible explanation.
As usual, a lot of knowledgeable posters. Thanks for your input.
Someone mentioned a Newton hotspot: do we know more about the positive residents? Where they live? where they work? their age?Would it be useful to know or intrusive?
@DW — May just be a coincidence, but testing limitations will leave some question marks. In general its not growing linearly (constant amount per day) but exponentially (constant percentage per day).
@Isabelle — HIPPA laws prevent disclosure of info on patients.
Updated with 4/1 data: http://newtonwatch.org/2020/03/29/covid-19-in-newton/
Jack, I’m with DW on this. No one is asking for names, but if the city was really doing contact tracing, 1) they should tell us what public places the infected people visited before they were diagnosed and 2) where they most likely picked up the virus. Otherwise raw numbers give us very little assistance. Thanks!
@Jack – Exponential growth is an idealized model for an epidemic; it breaks down pretty quickly when you mess with the random mixing of infected and susceptible persons – e.g. when you close schools, advise folks to work remotely, and so on. But the fitness of the model isn’t even relevant when we have no idea what proportion of the at-risk population is being tested.
In re: your other comment I would not think HIPAA has any bearing here. Can you provide any further detail? Thanks,
D
Sorry – Not random mixing, as who we encounter at school, work, etc is far from true random. But my point is that when a public authority tells a whole bunch of us to stay put, the resulting degree of mixing deviates from the idealized random a whole lot more.
@Arthur, did I actually say I think the public deserves more case level detail? I know I thought it. I think Isabelle gets the credit, but I certainly agree as well – unless there is a privacy law that supersedes public safety.
@Arthur — I think we all need to exercise universal precautions (like what came about in AIDS epidemic) and assume everyone (including ourselves) is infected and that all public surfaces are coated with the virus. Looking in the rearview mirror on where people got infected a week or two ago would just give a false sense of security and potentially unnecessary stigma to an establishment or organization (especially since most are closed now). It is not like we are dealing with a contaminated well or some point source. It is everywhere.
@DW — Unfortunately, exponential growth has proven to be a perfectly appropriate model for Covid-19 thus far. The world has been paralyzed thinking it was more complicated than that until last week. Different levels of distancing yield different characteristic growth rates. Over 33 days ago, when there were about 5000 cases worldwide. A simple 2-parameter exponential growth model predicted a million worldwide cases today. We’ll hit that tomorrow, and if India was included somewhat accurately, it would probably hit it today.
Let’s see where we are in Newton in 10 days on 4/11. We are a small population relative to the US or world, so things could jump around, but the data today says we’ll be around 300-400 cases depending on how much of the distancing and testing expansion impact has kicked in.
Here is some background on HIPAA
https://www.hhs.gov/hipaa/for-professionals/privacy/laws-regulations/index.html
Here’s a good article from the Globe indicating that we need to dig into the numbers and test more! Treating everything and everyone as contagious doesn’t answer the question about why the numbers are what they are-i.e. increasing despite more than two weeks of social distancing.
https://www.bostonglobe.com/2020/04/02/opinion/what-policy-makers-are-missing-coronavirus-data/
Yes, you are correct Jack. The basic principles of infectious disease epidemiology don’t disappear. The real challenges to seeing meaningful movement in the curve are: 1. The very small sample; 2. The short time interval; 3. Multiple distancing interventions over a 12 day period; 4. Dramatic ramp up of testing entirely within that period.
But @Jack’s two comments taken together paint the totality of the picture. The local epidemic is significantly larger than any reported number shows. If we did have more detailed case-locating information – and we should; nothing you shared, Jack, suggests that Public Health is an entity covered by HIPAA or that, as I alluded to earlier, public safety wouldn’t take precedence – we still could not be assured that the rest of the city (let alone Waltham, Watertown etc) was safe. We’re forced to take as much precaution as possible at all times.
If I have a moment later, I’ll try a stab at a quick calculation of how many cases we might actually have in Newton. Nothing fancy, but I’ve been meaning to do it.
@Arthur — It is an OK article but at bottom you see “Sunil Gupta is a professor of business”. To some extent he is just expressing armchair opinions like the rest of us.
The slow and limited testing in the US has been a huge problem (particularly the slow part) but I don’t think the picture we have is orders of magnitude off from reality. Korea did more in-depth testing of the population than anyone. That approach has helped them be more effective in containing the virus (along with starting much earlier than US).
But the South Korea case fatality rate is 169/9976= 1.69%? If they found loads of undetected cases relative to the rest of the world, this number should be much lower. The US CFR is currently 6063/244,433=2.48%. So maybe the US case count is low by a third, but its in the ball park. South Korea found that 95% of the people with Covid19-like symptoms had something else (Flu, etc). A lot of the people who are convinced they have Covid19 now in Mass have something else. As the testing circle moves outward from the clear cases, the hit rate goes down. Now it is possible that we are missing a lot of deaths as well as cases and that explains our relatively low CFR. Ultimately, we are only going to be sure of the extent of the problem by watching the ER flow into Newton Wellesley.
We were originally on track for 1100 cases in 9 days on April 11th. Now data is pointing to 384 give or take. Let’s work to drive it lower with more effective social distancing.
@DW — What further information would you want and how would it help? Perhaps spread could be traced to your favorite pub or local business or to your place of worship or to your child inadvertently spreading it to a dozen others with a resulting death? Unless it was recent enough for you to self-quarantine, it is not relevant.
“We’re forced to take as much precaution as possible at all times.”
Bingo. You’ve got it.
Plots for April 2nd added:
http://newtonwatch.org/2020/03/29/covid-19-in-newton/
Case counts aggregated at the zip code level
Clusters associated with commercial establishments (e.g. pharmacy, supermarket)
We’re all better off if when we know where to locate greater risk geographically and can then take steps to avoid or mitigate it. (That’s not at all to advocate any disclosure that could reasonably identify a person uniquely.) I’ve worked in the past with public release of HIV data; I’m pretty confident the city can safely share more usable information.
Having stats at the census tract level would be most useful.
Newton has a fair number of healthcare workers, Which may distort the data (more testing per capital, more essential worker status, less stay at home, higher infection rates). If exposure is happening in the workplace, where people live isn’t going to be as revealing.
Charlie Baker announces Massachusetts to start advanced COVID tracing program to help spread the disease. That’s what we need in Newton too!
“Gov. Baker says this is a much more robust and targeted approach that the state believes will be much more effective in slowing the spread of this highly contagious disease.”
“The tracing effort will be staffed by a team of epidemiologists and managed by the Bureaus of Infections Diseases and Lab Sciences. There will also be a virtual call center with 1000 virtual contact tracers.”
135 cases as of 4/4- Thank you city of Newton for a weekend update! – representing a bump of only 8 cases from the day prior (6% day-over-day growth). While the numbers bounced around – 13%, down to 8%, then up to 30% – over the past week, that volatility reflected more about testing than disease spread. And the average 15% for the 7 day period was clearly slower growth than the week prior. Perhaps we’re getting somewhere.
Here are updated plots: https://covid19.jackprior.org/2020/03/29/covid-19-in-newton-ma/
Here is a quick post on the slowing growth rate data in the EU that is driving today’s market optimism:
https://covid19.jackprior.org/2020/04/06/todays-optimism/
April 6th update. The curve is bending further.
https://covid19.jackprior.org/2020/04/06/todays-optimism/
I used Boston Marathon non-weekend to write a web app you can use to see Covid-19 trends and forecasts for MA and the rest of the US. The data is kept up to date automatically. Needs a bit more work to build in manually-entered Newton data.
http://app.jackprior.org
Give it a try. Works well on smart phones as well.
One thing you will notice is that current trends point to total deaths potentially exceeding total hospitalizations soon. Its non-intuitive and may reflect the number of deaths occurring in nursing homes with no hospital treatment.
Nicely done Jack!
One caveat that I tripped over and might not be immediately obvious. Each graph shows actual data on the left half and projected data on the right half – i.e. the projected data is just the continuation of the curve from the data on the left.
That’s perfectly reasonable representation but it means if the curve is rising on the left, it will always be rising forever into the future. i.e. this is very different than a model that estimates when the peak will begin to drop.